How I use Checklists in My Practice.
In 2012, I visited the late Dr Rakesh Sinha in Mumbai. Dr Sinha was not only a brilliant laparoscopic gynaecological surgeon but also an avid reader. He introduced me to the habit of reading. He also presented me with 3 books. One of it was “The Checklist Manifesto” written by Dr Atul Gawande, a surgeon in Harvard Medical School. It is one of the best books I have read. It changed the way I practiced work and life.
In his book Dr. Gawande told the story of how, after looking at the airline industry and the way airlines use checklists to make flights as safe as possible, he developed a surgical check list for safe surgeries while working with the World Health Organization.
Our brains can probably hold 5 or 6 items at one time. Beyond that, we will miss things. A checklist is a type of job aid used to reduce failure by compensating for the potential limits of human memory and attention. It helps to ensure consistency and completeness in carrying out a task.
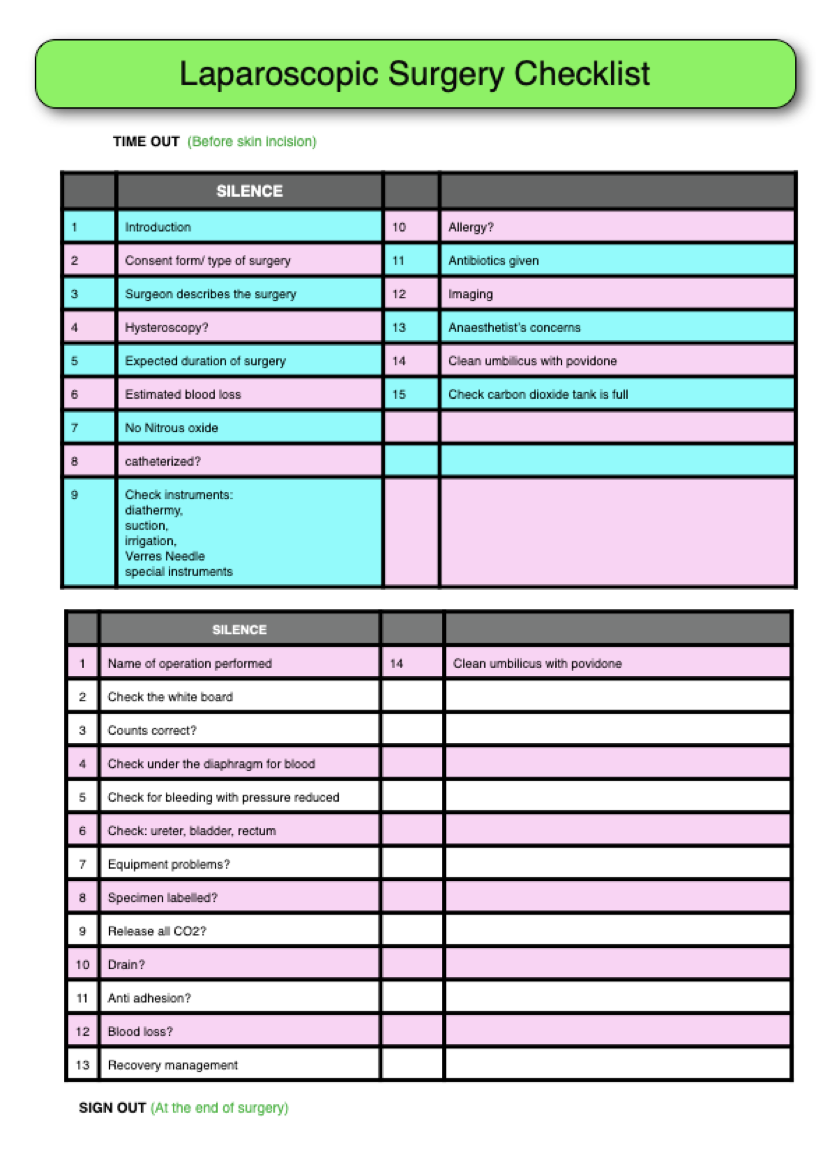
I started using checklists by implementing it in my operating lists. This, I actually started in 2012, even before the introduction of the WHO surgical checklist into our operating theatres. My first check list was for my laparoscopic surgeries. There are 2 parts to it: the first is the “time out” which is the checklist before starting a case and second is the “sign out” which is a check list used upon completion of the surgery, before closure of the wound.
The “time in” goes like this. It is similar to what was introduced by Dr Atul Gawande with some modifications for my practice.
1: Introduce yourself: Here everyone in the team will introduce themselves, starting with the surgeon: Dr Selva surgeon, the anaesthetist, my first, second and third assistants, the circulating nurse and the anaesthesist’s assistant and whoever is present in the operating theatre during the surgery. Even if my first assistant has been the same nurse assisting me for the last 15 years, we still go through the motion of introducing ourselves so that we know everyone by name.
2: Consent form/type of surgery. Here, the circulating nurse will read the consent form as to the type of surgery to be performed. This is very important especially to me, a gynaecological surgeon to ensure that I will be removing or repairing the correct organ.
3: Surgeon describes the surgery I will then describe the surgery. My team including the anaesthetist will understand what I am going to do during the procedure.
4: Hysteroscopy Since this is a personalised checklist for me, this is to remind myself whether I need to perform a hysteroscopy on the patient before the laparoscopy.
5: Expected duration of surgery. I will inform everyone, especially the anaesthetist, as to the expected duration of the surgery so that he can prepare the necessary drugs for the duration of the surgery.
6: Estimated blood loss. I will then mention the expected blood loss and to check whether any blood has been cross-matched for the surgery. If I have forgotten to get blood reserved for a surgery, this is an important reminder.
7: No Nitrous oxide. This item I placed in my checklist to remind the anaesthetist that during laparoscopic surgery, I do not like nitrous oxide administered as it causes swelling of the intestines, making my surgery difficult.
8: Cathetetrized? In some patients I prefer an indwelling catheter but in others, I just want the bladder to be drained without an indwelling catheter.
9: Check instruments Here, I will check several important instruments I use during the surgery.
The first is the diathermy. I will ensure that the diathermy machine is set up properly and working well, especially the bipolar diathermy.
After that I will check on the proper functioning of the suction irrigation system. A malfunctioning suction, can be disastrous during a surgery.
I will also check that the Verres needle is working well and that the insert and its sleeve are of the correct length.
Lastly I will ask for any special instruments I need during the surgery. This may include retrieval bags, special sutures, morcellators and so on.
I hate to be in a situation when the circulating nurses only start looking for instruments when the surgery has commenced. It is best to have all the things needed, available in the operating theatre before I start the surgery.
10: Allergy? The team is reminded of the allergies the patient is suffering from.
11: Antibiotics given? This is to ensure that the appropriate antibiotics have been given prior to commencing the surgery.
12: Any imaging? Sometimes I may have MRI or ultrasound images that may need to be displayed during the surgery.
13: Anaesthetist concern. I will ask the anaesthetist whether he has any worries about the patient before commencing the surgery. I have been, on occasion surprised to learn something I hadn’t known about the patient, from the anaesthesist.
14: Clean umbilicus with povidone-iodine. This is again to remind myself that the umbilicus must be very clean before starting the surgery. In most laparoscopic surgeries, the first incision is through the umbilicus and there is a high risk of infection in the umbilicus if it is not cleaned properly.
15. Check carbon dioxide tank is full. This is important because I do not want to disrupt my surgery because of an empty carbon dioxide tank. If the tank is not full I will ask for another tank to be placed in the operating theatre so that switching of the tank can be done quickly, without any disruption.
This is my preoperative checklist before I start any laparoscopic surgery. I also have similar checklists for my open or laparotomy surgeries as well as Caesarean sections.
Dr Gunasegaran pointed out one more item I need to include in this time out checklist and that is whether I may “need assistance of a general surgeon or a urologist” during the surgery. This will be a reminder to inform them that I will be starting the case and I may call them if needed during the surgery.
The next and equally important check list is the “sign out” checklist, which is done once the surgery is over and before closing the skin.
The first thing the circulating nurse will say is “silence” so that every one stops what they are dong and listens to her.
1: Name of operation performed I will announce the surgery we had just completed to confirm it matches what is written on the consent form.
2: Check the white board. There is a white board in the operating theatre on which, during the surgery , I will be asking my circulating nurse to write down things that I need to check at the end of the operation. Some of the things that may be written include the total number of fibroids removed, gauze that is placed in the abdomen and so on. This is to remind me to check these items before closing the abdomen.
3: Counts correct? Here the assistant nurse will check all needles, swabs and instruments used during the surgery to ensure that all counts are correct and nothing is missing.
4: Check under the diaphragm for blood. During gynaecological surgeries blood gets trapped under the diaphragm and it is easy to forget to aspirate this blood. This is a reminder to do so.
5 Check for bleeding with pressure reduced. Increased intraabdominal pressure during surgery could mask bleeding, especially of major pedicles. This is to remind me to reduce the intraperitoneal pressure and check the pedicles to ensure that there is no bleeding.
6: Check ureter, bladder and rectum. Again this is to ensure that all these organs are intact and not injured during the surgery.
7: Equipment problems? Here, we will check to ensure that all the instruments used during the surgery are still in good working order. If we break an instrument or find that the diathermy is faulty, this will be recorded and the operation theatre sister will be informed.
8: Specimen labelled This is to ensure that all specimens removed are bagged and labelled correctly and that nothing is missing or misplaced.
9: Release all Carbon dioxide Leaving carbon dioxide in the abdomen after laparoscopic surgery may lead to postoperative discomfort. This is a reminder to release all the carbon dioxide from the abdomen before closing.
10: Drain? Some patients may require a drain in the abdomen. This is to remind me whether a drain is needed for the patient.
11: Antiadhesions? Some patients may require antiadhesion gel or powder to prevent postoperative adhesions.
12: Blood loss? The blood loss that occurred during the surgery is recorded.
13: Recovery management Both the anaesthesist and I will decide whether the patient will require any special attention while in the recovery bay. – whether the patient needs more blood transfusion, admission to ICU and so on.
14. Clean umbilicus with povidone-iodine A reminder to clean the umbilicus again thoroughly before closing, to prevent any infection in the umbilicus.
I have been using this checklist since 2012 and despite using this list, we have still have made mistakes during surgeries. Mistakes happen when one of us in the team becomes lackadaisical in enforcing the checklist diligently. The commitment is to do the checklist all the time, even in emergency cases. I always tell my team that the responsibility lies with the circulating nurse. She must be firm to ensure that the checklist is done before and after every surgery. Sometimes, a new circulating nurse will find it a daunting task to tell the surgeon and anaesthetist to stop and listen to her go through the checklist. I even have my checklists translated to Malay (Bahasa Malaysia) for nurses who are not proficient in English. In some operating rooms these checklists are fixed on posters attached to the walls in the operating room.
Having established this checklist for all my operations, I decided to extend it to my daily life. I have a checklist before I leave the house every morning to ensure that I have done and taken everything before going to work. When I sit at my desk in my clinic, I have a checklist to start my morning routine. This includes writing my journal, checking my calendar to see what I have in store for myself for the day and so on. I also have a checklist for anything new I do. For example, I recently started HIFU or High Intensity Focused Ultrasound services in my hospital and before I start a case I have a check list to ensure that I am doing every thing in a systematic manner. One of my most treasured checklists is my “travel checklist” whereby I have a list of things I will check before leaving Melaka to the airport in Kuala Lumpur. I don’t want to forget anything as the consequences may mean, missing a flight.
So what I advice can I give doctors going into private practice
- If possible read the book “The Checklist Manifesto” abd AHO Safe surgery checklist.
- Start by first creating a checklist for the most important part of your work namely before starting surgery. Then, incorporate checklists into your daily life. It will remove a lot of stress in your daily routine
- Always revisit your checklist and improve on it. After sometime, when you are too comfortable with your checklist, you may think that you know it so well that you don’t have to go through it one item at a time. This is when you will make a big mistake for trusting your memory. Keep revisiting the list to ensure that you follow all the points diligently every time even if you think you know it by heart.
- Inculcate the culture of safe surgery in the operating theatre among your colleagues
- Take time to teach and train your nurses in the operating theatre and clinic and it is effort well spent
Selva
17/4/2022
Acknowledgements
I would like to thank my wife Sarojini for editing this article
I would also like to thank Dr. Gunasegaran for reading through this article and giving good suggestions.