There are several techniques in performing surgery for ectopic pregnancy
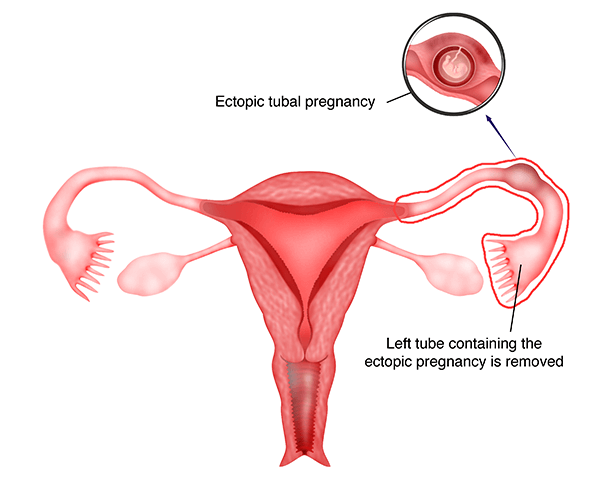
1) Laparoscopic Salpingectomy
This technique involves the excision of the tube containing the ectopic pregnancy. It can be performed using the 3 or 4 port technique or a single incision technique. In the 3 or 4 port technique, the tube is held with a grasper and the mesosalpinx (the tissue that holds the tube to the uterus) is coagulated using bipolar current, and then cut. The tube containing the ectopic pregnancy is then detached from the uterus and the ovaries.
Care must be taken to be as close to the tube as possible because sometimes, excessive coagulation can cause the blood supply to the ovaries being compromised.
In ruptured ectopic pregnancy, there may be active bleeding and this bleeding has to be coagulated first before attempting to excise the tube. Blood and blood clots present in the abdominal and pelvic cavity have to be aspirated and this can sometimes be a tedious problem.
The ectopic tissue is then placed in a bag and removed from the pelvis. Copious irrigation of the pelvis and abdomen is done to remove all the blood accumulated in the pelvis.
The advantage of laparoscopic salpingectomy is that the tube with the ectopic pregnancy is removed and so there will be no worry of some ectopic pregnancy tissue left in the pelvis.
The disadvantage is that the removal of the tube reduces the chances of spontaneous pregnancy. If the other tube is patent, the patient still has a chance of spontaneous pregnancy. However, if this tube is blocked or damaged, she will only be able to conceive via invitrofertilization (IVF).



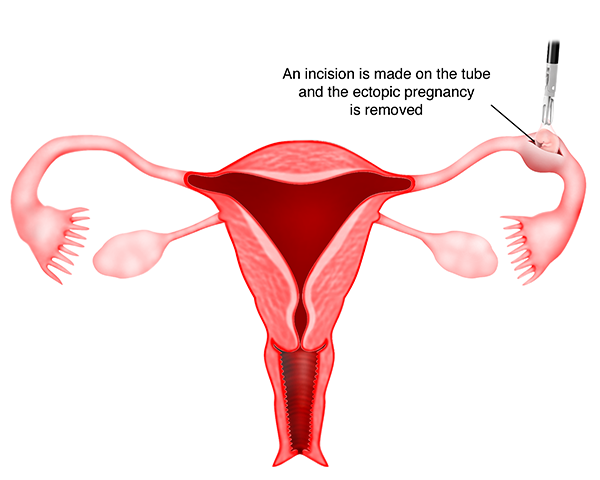
2) Laparoscopic Salpingotomy
In this technique, an incision is made on the antimesenteic border (g) ( the part of the tube that is opposite to the mesosalpinx (g)) of the fallopian tube, and the ectopic tissue is extracted from the tube. The incision on the tube may or may not be sutured.
If the incision is sutured, the surgery is called laparoscopic salpingotomy. If the incision is not sutured than the surgery is called laparoscopic salpingostomy. This technique is usually performed on unruptured and early tubal pregnancy.
The advantage of this technique is that the tube is still intact and so the patient can conceive with the assistance of this tube in the future.
The disadvantage is that, because the tube is scarred as a result of the surgery, another ectopic pregnancy may occur at the same site. There is also a small risk that after the surgery, some ectopic pregnancy may still be present in the tube and this may grow.
As such, if this technique is performed it is essential to repeat the blood test (serum beta HCG) to ensure that the level is declining, thus indicating that there is no further growth of the ectopic pregnancy. A hysterosalpingography will be required after 3 months to ascertain whether the tube is still patent. This technique is usually recommended if the patient only has 1 patent tube because removal of the tube will necessitate IVF for the patient to conceive.

Case 26.1
Spontaneous pregnancy after Laparoscopic Salpingotomy for an Ectopic Tubal Pregnancy
NMA, a 33-year-old lady first consulted me in 2013. She was eight weeks pregnant. Ultrasound showed 2 well-formed gestational sacs with fetuses but with no fetal activity. She underwent a suction curettage. Postoperatively, she was well with regular menstrual periods. Six months later she presented with pelvic pain. She had missed her menses and a pregnancy test was positive. Ultrasound showed a normal sized uterus with no intrauterine gestational sac and a left adnexal mass with fluid in the Pouch of Douglas. A diagnosis of ectopic pregnancy was made. She underwent a laparoscopic salpingotomy (watch video 26.2). Postoperatively she was well. She underwent a hysterosalpingogram (HSG) six months later, which showed a patent right tube. The left tube could be seen but there was no spillage of dye. She underwent one cycle of intrauterine insemination but it was without success. She conceived spontaneously four months later and delivered a healthy baby girl in 2015.
Discussion
The 2 types of surgery that can be done for tubal ectopic pregnancy are (1) laparoscopic salpingostomy and (2) laparoscopic salpingectomy. Laparoscopic salpingostomy can only be done if the fallopian tube is not ruptured. The advantage is that, the patient will still have the tube although it is diseased. She may be able to conceive spontaneously with the operated tube. This method is usually considered when a patient only has 1 normal tube and has developed an ectopic pregnancy in that tube. NMA was keen to retain the tube and so a salpingotomy was done. She would have run a risk of developing a second ectopic pregnancy in the operated tube but fortunately, she conceived with an intrauterine pregnancy and delivered the child.
3) Laparoscopic excision of cornual pregnancy
When the ectopic pregnancy is at the cornual region of the
uterus (Figure 7.4), then pregnancy is usually diagnosed much later. Cornual pregnancy is much more difficult to excise laparoscopically because it is larger and can bleed extensively. The technique involves injection of vasopressin around the cornual ectopic pregnancy and placing a purse string suture around it. An incision is then made to enucleate the ectopic pregnancy. The defect is then sutured. In large cornual pregnancy, a part of the uterus may have to be removed together with the tube. In difficult cases, laparotomy may be necessary.

Case 26.2
Laparoscopic Resection of a Cornual Ectopic Pregnancy
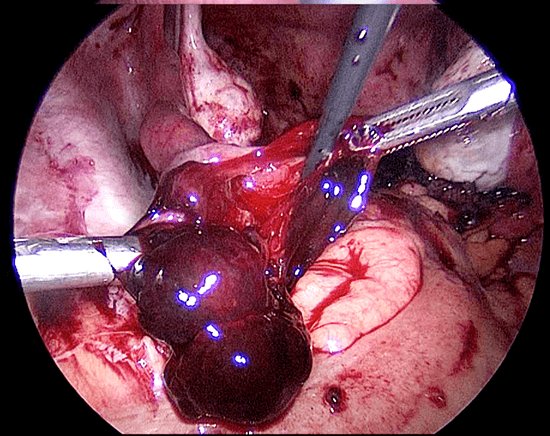
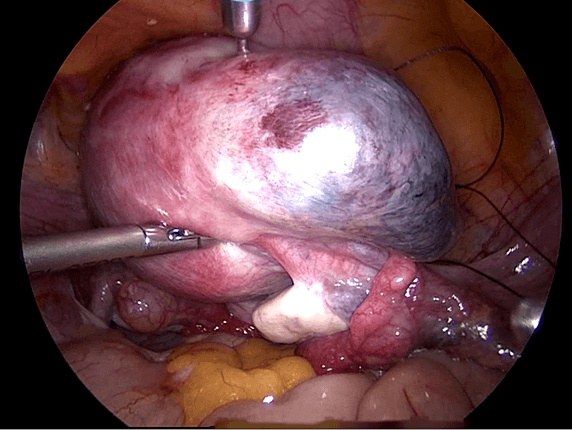
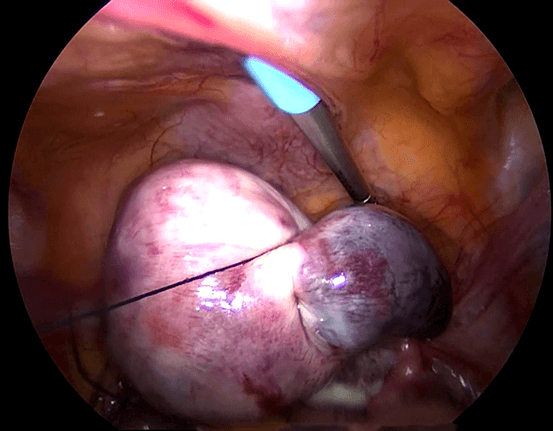
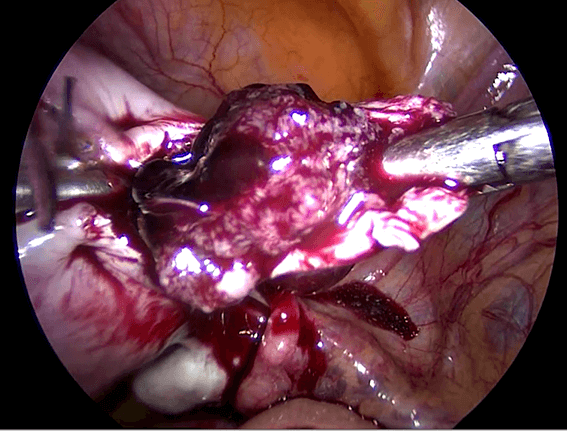
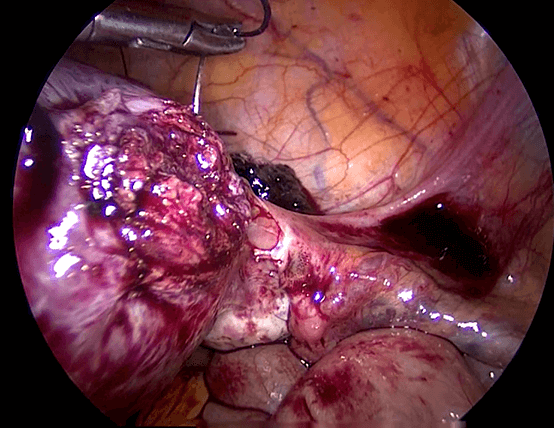
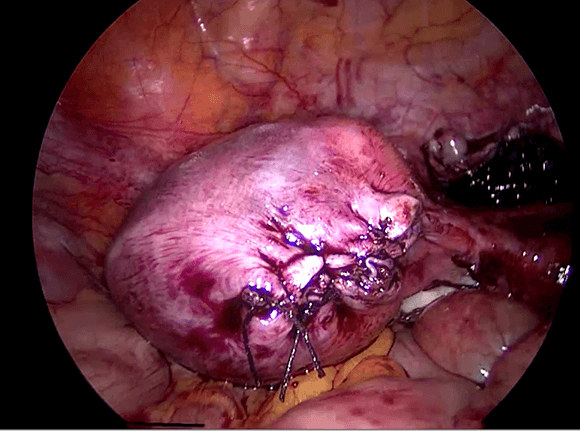
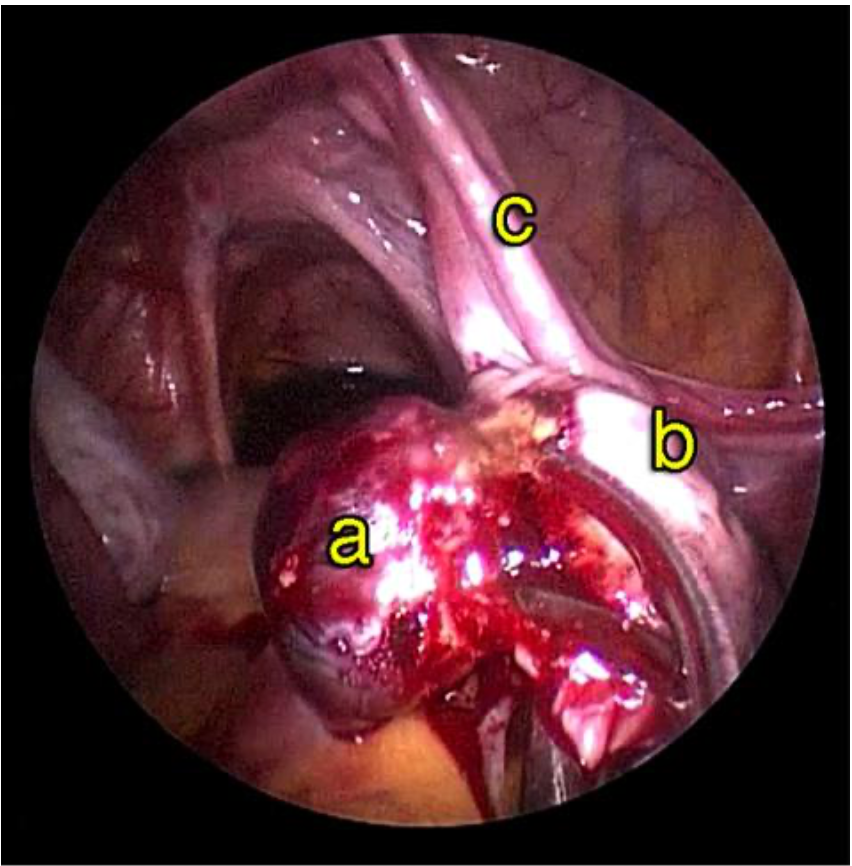
Madam UDS who had been married for 3 years came to see me in 2009 because she was unable to conceive. Hysterosalpingogram done in another hospital showed that both her tubes were blocked. She underwent a laparoscopy, which showed a normal sized uterus. Both her tubes were normal and were patent after tubal insufflation was performed under pressure. She conceived spontaneously 2 months after the laparoscopy but unfortunately, it ended as a missed abortion. She had to undergo an evacuation of the product of conceptus. Postoperatively, she was well but could not conceive. She was given several cycles of clomiphene citrate with no success. In 2011, she underwent an intrauterine insemination cycle after being given follicular stimulating hormone (FSH) injections. She conceived after the procedure. Unfortunately it resulted in a cornual ectopic pregnancy. She underwent a laparoscopic right cornual resection of the ectopic pregnancy in 2011 (Figures 26.7 -26.11) (watch video 26.3). Post operatively in 2013 she underwent a hysterosalpingography, which showed that the left tube was not patent. She conceived after undergoing IVF.
Discussion
Cornual ectopic pregnancy is not common. It is usually diagnosed late because patients with this condition do not have many symptoms. Rupture of a cornual ectopic pregnancy can lead
to profuse bleeding. In this patient, the diagnosis was done early because she underwent an IUI and was on regular follow- up. The excision was done successfully laparoscopically.
4) Laparoscopic Excision of Ovarian Ectopic Pregnancy
Ovarian ectopic pregnancy is rare. When the ectopic pregnancy is in the ovary, the ectopic pregnancy and a small part of the ovary, has to be excised. This has to be done carefully to ensure that all the ectopic pregnancy is removed and not too much ovarian tissue is removed with it.

5) Single Incision Laparoscopic Surgery for Ectopic Pregnancy
A number of the above mentioned surgeries can be performed by using the single incision laparoscopic technique. Although the surgery performed is the same, the technique involves only one incision through the umbilicus. This is technically more demanding for the surgeon. Laparoscopic salpingectomy for tubal ectopic pregnancy and even the excision of ovarian ectopic pregnancy is currently performed using single incision laparoscopic surgery.

Summary
Laparoscopic surgery for ectopic pregnancy includes laparoscopic salpingectomy, laparoscopic salpingotomy, laparoscopic excision of cornual pregnancy and laparoscopic excision of the ovarian ectopic pregnancy. All these procedures can also be performed using the single incision laparoscopic method.