Laparoscopic surgery for ovarian cysts will depend on the type of cyst. Generally, non-pathological cysts (follicular and corpus luteal cysts – see Chapter 5) do not require surgery except when there is a complication (torsion, bleeding etc).
Endometriotic cysts have been discussed in Chapter 25 and polycystic ovarian disease in Chapter 23. Laparoscopic surgery for the most common benign pathological cysts namely the dermoid cyst and benign cystadenomas is discussed in detail below:
Laparoscopic surgery for benign pathological cysts
1) Laparoscopic Cystectomy (removal of the cyst)
This the commonest surgery performed for a benign cyst like a dermoid cyst. The surgery involves removal of only the cyst and leaving normal ovarian tissue behind. The skill of the surgery is to separate the cyst from the ovary without spillage.
How is Laparoscopic Cystectomy performed?
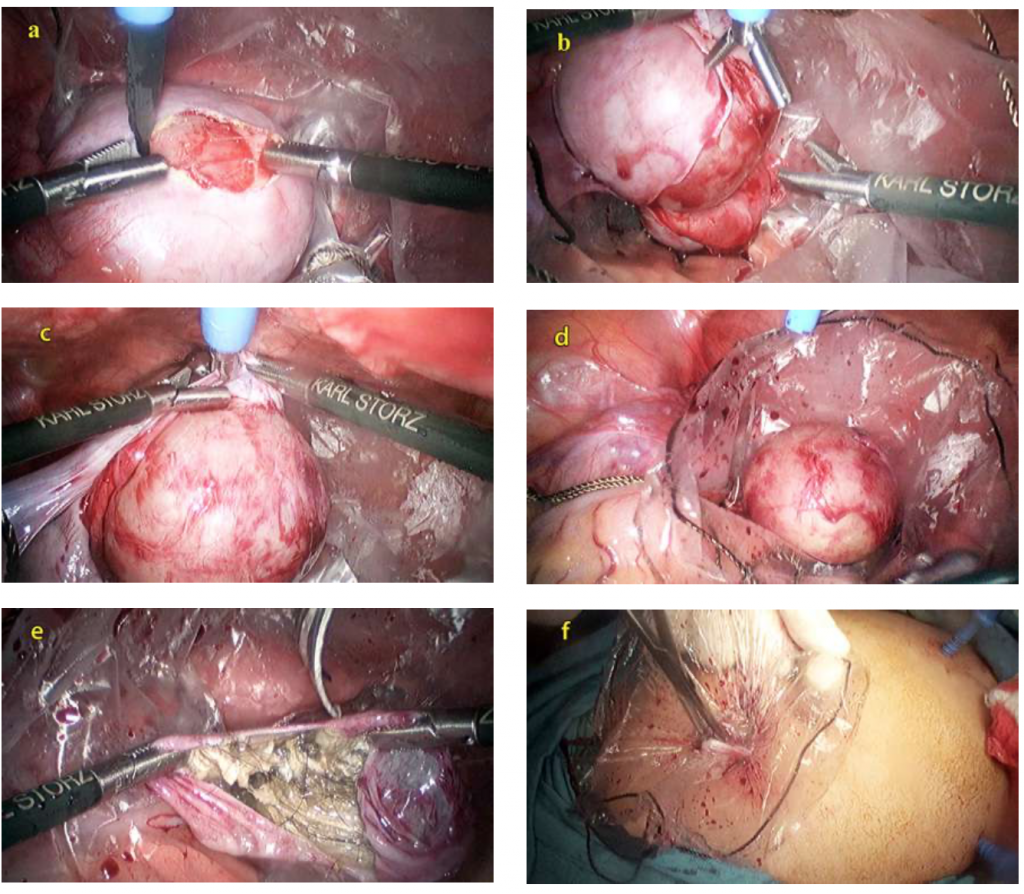
This surgery is performed by first placing the cyst in a bag which is placed in the pelvic cavity. The bag will help collect any spillage, which may occur if the cyst is accidentally opened during the cystectomy.
An incision is made on the cyst to separate the cyst from the ovary. By gentle dissection, it is possible to completely separate the cyst intact from the ovary. However, as cyst walls can be very thin or densely adherent to the ovary, sometimes a hole can be made in the cyst. If this occurs, the contents of the cyst can be aspirated and a cystectomy is performed, with the ovary still being within the bag.
The bag (with the cyst and its contents) is then closed and removed through a slightly enlarged incision in the umbilicus. The pelvis and abdomen are then thoroughly washed. If the defect in the ovary is large, the ovary may be repaired with sutures.
In patients who wish to conceive, the patency of the fallopian tubes will be tested. If there are other incidental findings such as adhesions or endometriosis, these will be treated as well.


What are the advantages of a Laparoscopic Cystectomy?
All the advantages of laparoscopic surgery described in chapter 15 also apply to laparoscopic cystectomy. However, many women with dermoid cysts are young and will desire pregnancy in the future. Laparoscopic cystectomy will reduce the incidence of postoperative pelvic adhesions, thus the chances of spontaneous pregnancy is perhaps higher after laparoscopic cystectomy compared to conventional cystectomy performed by laparotomy.
What are the disadvantages of Laparoscopic Cystectomy?
The contents of a dermoid cyst are varied (hair, teeth, thick paste like (sebaceous) material, watery fluid). Spillage of these cyst contents into the pelvis and abdomen can cause postoperative pain, adhesion and may also cause difficulty in conceiving. Performing laparoscopic cystectomy for dermoid cyst without spillage of its contents in the pelvis and abdomen is a skillful surgery. When the surgery is performed within a bag, the chance of spillage of its contents into the pelvis and abdomen, is reduced. Technically, the bigger the cyst, the more difficult the surgery.
2) Laparoscopic Salpingoophrectomy (Removal of the ovary and tube)
In older women who have completed their families, a second option is to remove the whole ovary. This can be done especially if the ovary is very large. In a large dermoid cyst, cystectomy may be difficult to perform and the amount of remaining normal ovarian tissue will be small. Laparoscopic salpingo- ophrectomy is a much easier operation to perform compared
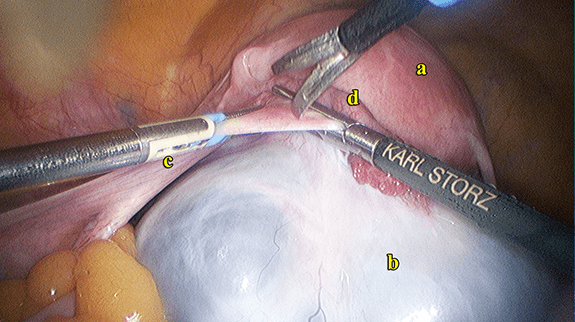
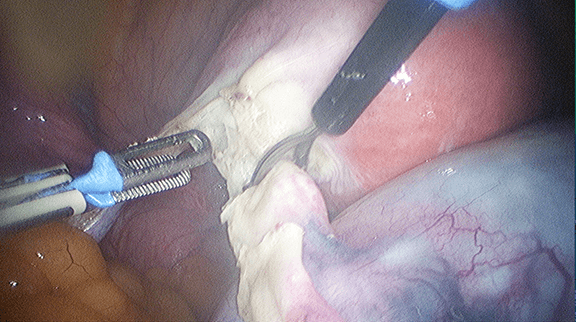
to laparoscopic cystectomy. The surgery is performed by
first detaching the ovary from its blood supply by isolating, coagulating and cutting the infundibulopelvic ligament (the ligament that contains the blood supply to the ovary). The ovary is then detached from the uterus by coagulating and cutting the ovarian ligament (the ligament that is attached to the uterus). The ovary that has been detached is placed in a bag. The fluid in the cyst is aspirated, and the bag is closed and removed usually through an enlarged incision made in the umbilicus. The pelvis and abdominal cavity are then thoroughly washed.

Case 27.1
Laparoscopic Salpingoophrectomy and Omentectomy for Ovarian Cancer
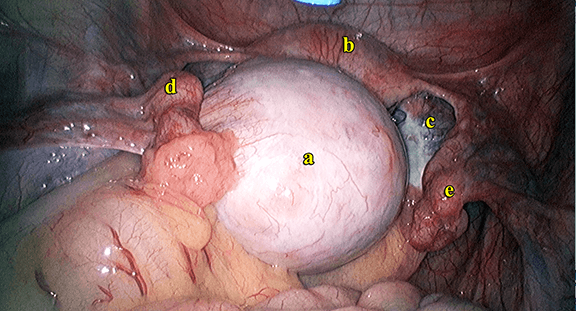
TS, a 43 year old lady, has been married for 21 years with no children. She had 3 unsuccessful IVF cycles. She was diagnosed with an ovarian cyst in another hospital. She had undergone a lumpectomy and axillary node clearance for a left breast cancer 2 years earlier. She also received radiotherapy and chemotherapy for the breast cancer. Examination
and ultrasound showed a mixed echogenic cyst (containing both solid and cystic structures) measuring 4.65 x 3.44 cm. There were small cysts in the right ovary as well measuring 1.08 x 1.23 and 1.15 x 1.72cm. There was minimal fluid in the Pouch of Douglas. A PET scan done was normal. Both she and her husband were counseled regarding the possibility of the mass being a metastatic breast cancer. She wanted a conservative surgery and still wanted to conceive. She underwent a laparoscopy. The right ovarian tumour (Figure 14.1) appeared malignant whereas the right ovarian cysts appeared benign. The right ovary was removed and sent for frozen section. Biopsies of the left ovary and partial omentectomy were also done. The histopathology was an adenocarcinoma probably metastatic from the breast cancer. Postoperatively she recovered well. Further histopathological assessment of the ovarian mass and comparing it with that of the breast cancer concluded that the ovarian tumour was not a metastatic cancer of the breast but a primary ovarian cancer. She is currently contemplating removal of all the reproductive organs.
Discussion
Laparoscopic surgery for ovarian cancer is a controversial topic. Most of the ovarian cancer cases are performed by laparotomy. In this case, since she was not mentally prepared to remove of both her ovaries and the uterus, laparoscopy was performed to make a diagnosis of the pelvic tumour and then contemplate further surgery. Laparoscopy aided in avoiding multiple laparotomies.
3) Laparoscopic Hysterectomy
On rare occasions, a dermoid cyst can be cancerous. This will not be known until a pathologist examines the cyst. Older women with a dermoid cyst have a higher chance of it being malignant. Thus, in women who are above 45 years of age, a hysterectomy and removal of the ovary with the cyst or both ovaries is another option. Laparoscopic hysterectomy is discussed in Chapter 33.

4) Single incision Laparoscopic surgery
All the above-mentioned surgeries can also be performed with a single incision. Single incision laparoscopic salpingo- ophrectomy (removal of the ovary) and hysterectomy (removal of the uterus) are fairly easy to perform. However, single incision laparoscopic cystectomy can be more challenging especially in patients with large cysts. (see chapter 19)



Summary
Laparoscopic surgery for an ovarian cyst will depend on the type of cyst. The surgeries that can be performed are laparoscopic cystectomy, laparoscopic salpingoophrectomy and laparoscopic hysterectomy. All these surgeries can also be performed by single incision laparoscopy.