Surgery for endometrial cancer has been traditionally performed by laparotomy. Nowdays, Hysterectomy and Pelvic Lymphadenectomy can be performed laparoscopically.
Advantages of Laparoscopic surgery for endometrial cancer
All the advantages of laparoscopic surgery discussed in chapter 15 also apply to this type of surgery. Some of the special advantages are:
1) Magnification makes the surgery easier and more precise to perform.
2) It can be used as a tool to explore the pelvis and abdomen to stage the disease. Biopsies can also be taken from any part of the pelvis or abdomen.
3) In patients who are found to have more advanced cancer, laparoscopy provides the advantage of a quicker postoperative recovery and thus allowing an early start of radiotherapy and/or chemotherapy.
Risks of laparoscopic surgery
1) There is always a slight worry that laparoscopic surgery itself may cause spread of the disease because of the use of carbon dioxide to distend the abdomen. However this fear has been allayed by numerous studies that have been performed on laparoscopic surgery in cancer treatment which state that laparoscopy is safe for cancer surgery.
2) In some cases when the disease has spread or is adherent to vital structures such as bowel or blood vessels, it may not be possible to perform the surgery laparoscopically and so a laparotomy may have to be performed.
Suitable candidates for laparoscopic surgery
Patients with early Cancer of the Endometrium are best suited for laparoscopic surgery. These patients can benefit from all the advantages of laparoscopic surgery because cancer of the endometrium is often diagnosed early.
The technique
There are three basic aspects of laparoscopic surgery for cancer of the endometrium. They are:
1) Laparoscopic hysterectomy
2) Pelvic Lymphadenectomy or pelvic lymph node sampling 3) Para-aortic lymph node sampling
1) Laparoscopic hysterectomy
Laparoscopic hysterectomy is described in detail in Chapter 33. There is a slight difference when performing laparoscopic hysterectomy for Cancer of the Endometrium. In order to reduce haemotogenous (spread through the bloodstream) dissemination of the cancer, both the fallopian tubes and the infundibulopelvic ligaments are coagulated at the beginning of the surgery. Isolation and ligation of the uterine arteries at its origin from the internal iliac arteries follow. The spaces in the lateral pelvic wall are then opened to see if there are any enlarged lymph nodes. If enlarged lymph nodes are seen, these are removed and sent for frozen section (g). The pelvic lymphadenectomy
can be performed before or after the hysterectomy. The hysterectomy is then performed as described in Chapter 33.
2) Pelvic Lymphadenectomy or Pelvic Lymph Node Sampling
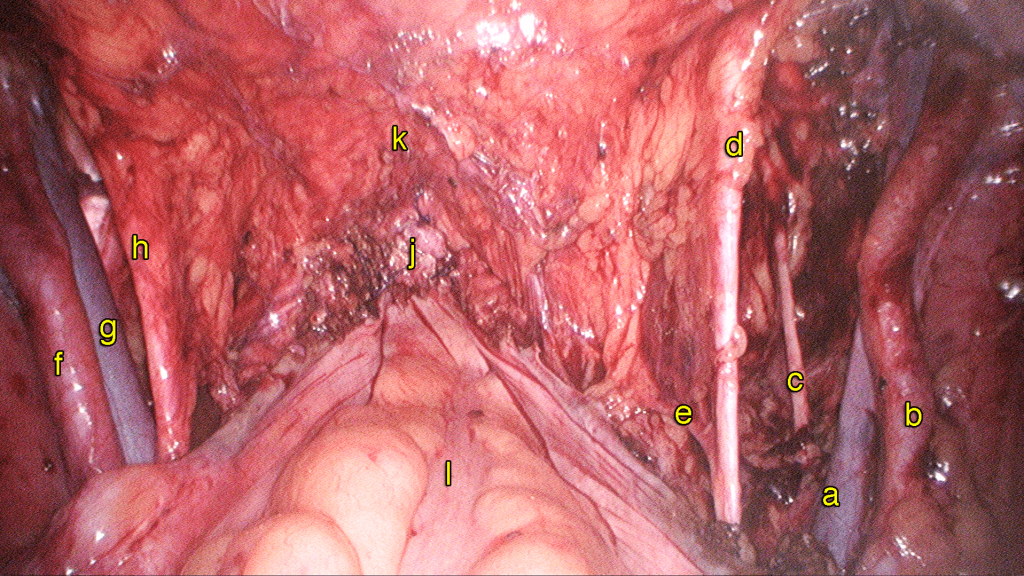
Pelvic Lymphadenectomy is performed by first opening up of the space around the vessels of the pelvis, namely the common iliac vessels, the external iliac vessels, the internal iliac vessels and the obturator vessels, the lymph nodes surrounding these vessels are removed.

Total laparoscopic hysterectomy and pelvic lymphadenectomy for endometrial cancer
http://vimeo.com/159032432
Case 34.1 Cancer of the endometrium: Total Laparoscopic Hysterectomy and Bilateral Salpingoophrectomy and Pelvic Lymphadenectomy
Madam LLH, a 55-year-old had postmenopausal bleeding. She underwent a hysteroscopy and a Dilatation and Curettage in a different country. The histopathology confirmed a well differentiated endometriod adenocarcinoma. Examination and ultrasound done showed a normal sized uterus. She underwent a Total Laparoscopic Hysterectomy and Bilateral Salpingoophrectomy and Pelvic Lymphadenectomy. The surgery took 2 hours (watch video 34.1). Postoperatively she was well. The histopathology confirms moderately differentiated adenocarcinoma with no pelvic lymph nodes involvement. She did not require any additional chemotherapy or radiotherapy. She is currently on followup.
3) Para-aortic lymph node sampling
Laparoscopic para-aortic lymph node dissection is a technique whereby lymph nodes are removed from around the aorta and vena cava. The removal of para-aortic lymph nodes is a controversial complex surgery which is not routinely performed. It requires a surgeon with advanced laparoscopic skills.
Summary
• Laparoscopic surgery can be performed for endometrial cancer.
• Total laparoscopic hysterectomy and pelvic lymphadenectomy are usually performed together.
• Performing this type of surgery laparoscopically requires advanced laparoscopic skills