Diagnostic hysteroscopy is performed to make a diagnosis of a symptom (see Figure. 36.1)
Indications for Diagnostic Hysteroscopy
Diagnostic hysteroscopy is performed for the following reasons
1) Evaluation of abnormal vaginal bleeding
2) Evaluation of unusual vaginal discharge
3) Evaluation of infertility
4) Location of a foreign body (eg intrauterine contraceptive device)
5) Evaluation of repeated miscarriage
6) Evaluation of abnormal transvaginal ultrasound
7) Evaluation of an abnormal hysterosalpingogram (HSG)
8) Preoperative evaluation
9) Postoperative evaluation
10) Diagnosis and classification of a submucous fibroid
11) Diagnosis and staging of endometrial cancer
How is it performed?
A Diagnostic Hysteroscopy is usually done without any anaesthesia and as an outpatient procedure. This procedure is sometimes called Office Hysteroscopy. A simple oral painkiller may be given before the surgery. A fine telescope attached to a camera is inserted into the uterine cavity via the cervix. Saline or carbon dioxide is used to distend the endometrial cavity so that there is space for the cavity to be visualised. This endometrial cavity can then be seen on a video monitor. The patient can see the procedure while it is being done. Some patients may experience discomfort while the surgeon negotiates through the internal Os (the junction between the cervix and the uterine body) into the uterine cavity. Fine surgical instruments may be then passed into the uterus to perform minor surgery such as taking a small sample of tissue (biopsy) of the endometrium, releasing adhesions or removal of polyps. The procedure usually takes between 5 to 10 mins.
Advantages of Diagnostic Hysteroscopy
Outpatient or office procedure – A diagnostic hysteroscopy can be performed without anaesthesia as an outpatient or office procedure.
The endometrial cavity can be visualised directly and a diagnosis can be made immediately.
Some minor surgery can also be performed at the same time.
Preoperative preparation
The best time to perform a diagnostic hysteroscopy is just after menses. At this time the endometrial lining is very thin and not vascular. No preparation is usually required. An oral painkiller (analgesic) may be given 30 minutes before the procedure. When a tight cervical Os is anticipated (eg postmenopausal women) a tablet (misoprostol – cytotac) may be given orally or placed in the vagina 30 minutes before the procedure. A local anesthetic may sometimes be injected into the cervix before the procedure.
Minor surgeries that can be performed during diagnostic hysteroscopy
1. Biopsy (a small sample of tissue is taken) of the endometrium
2. Removal of small endometrial polyps (see Chapter 6)
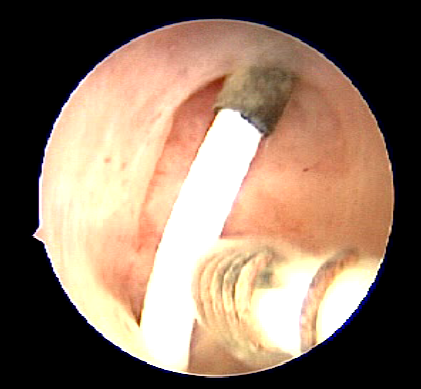
3. Removal of a missing IUCD (Figure. 37.1).
4. Release of endometrial adhesion

Summary
Diagnostic hysteroscopy is a very useful tool in the evaluation of the endometrial cavity when endometrial pathology is suspected. It can be done without anaesthesia in an office setting