What are the advantages of Laparoscopic Hysterectomy?
The advantages of laparoscopic surgery are the same as the advantages described in chapter 15.
What are the dangers of Laparoscopic Hysterectomy?
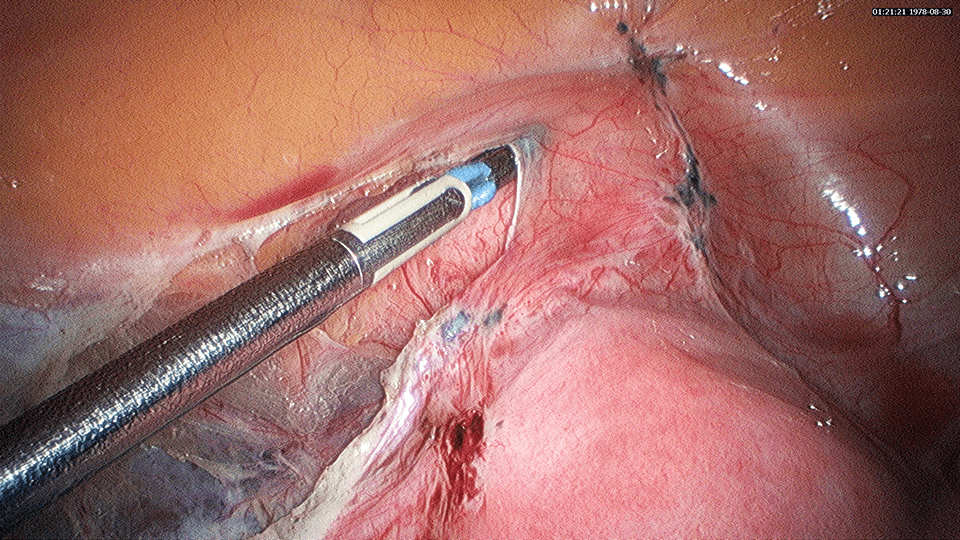
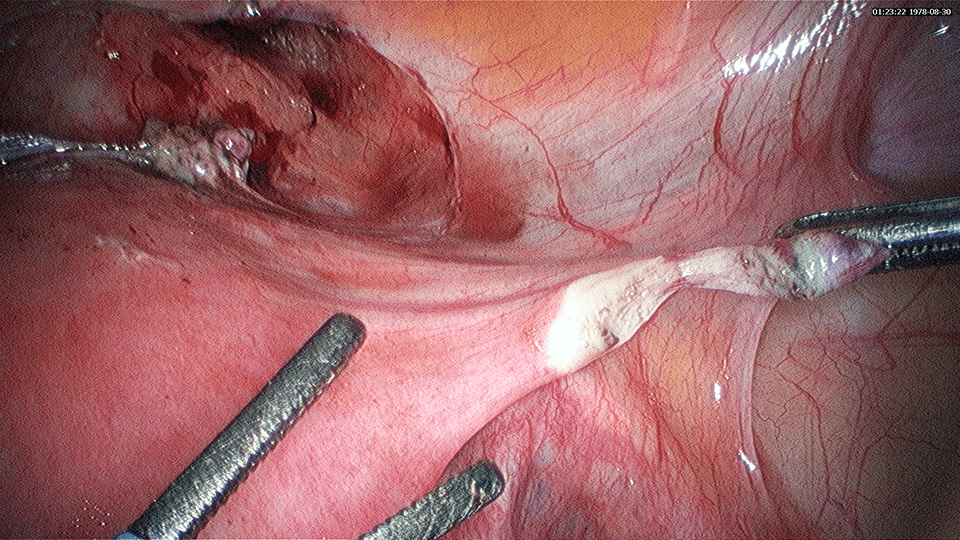
Laparoscopic Hysterectomy involves the detachment of the uterus from the pelvis. There are certain important structures that are nearby or attached to the uterus that may be accidentally injured during the surgery. These structures include the ureters, bladder and the bowel. If injury is recognized during the surgery, repair can be done. The injury is sometimes only noted after the surgery and a second surgery may be necessary to repair the injured structure such as a ureter.
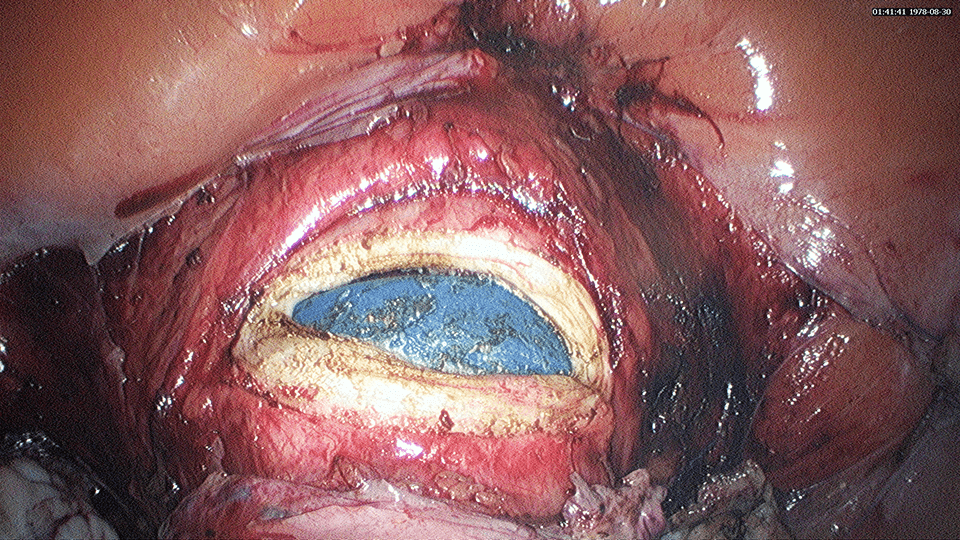
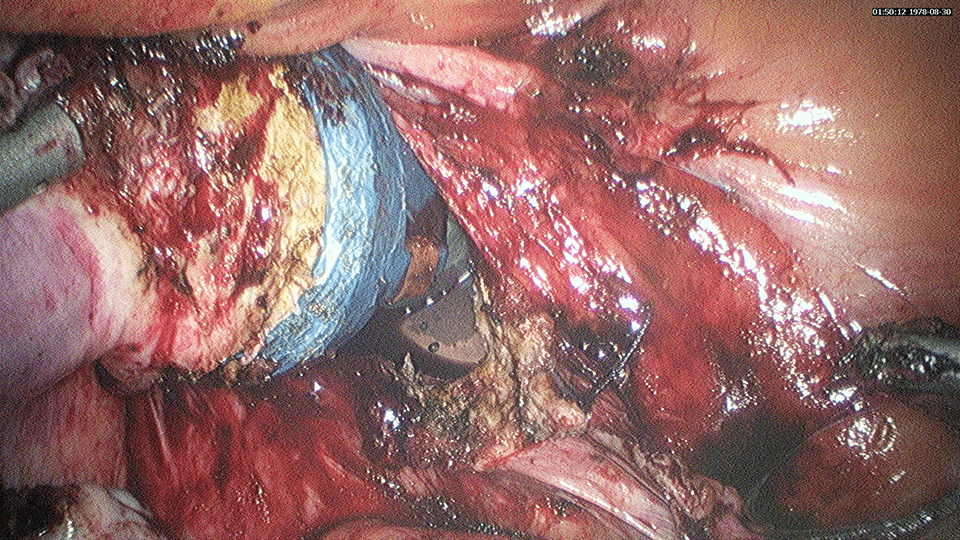
The Bladder is located in front of (anterior to) the uterus and cervix. Due to diseases such as endometriosis or a previous Caesarean section, the bladder sometimes may be adherent to the uterus. In such situations, injury to the bladder may occur. Repair of the bladder may be necessary either laparoscopically or by a laparotomy.
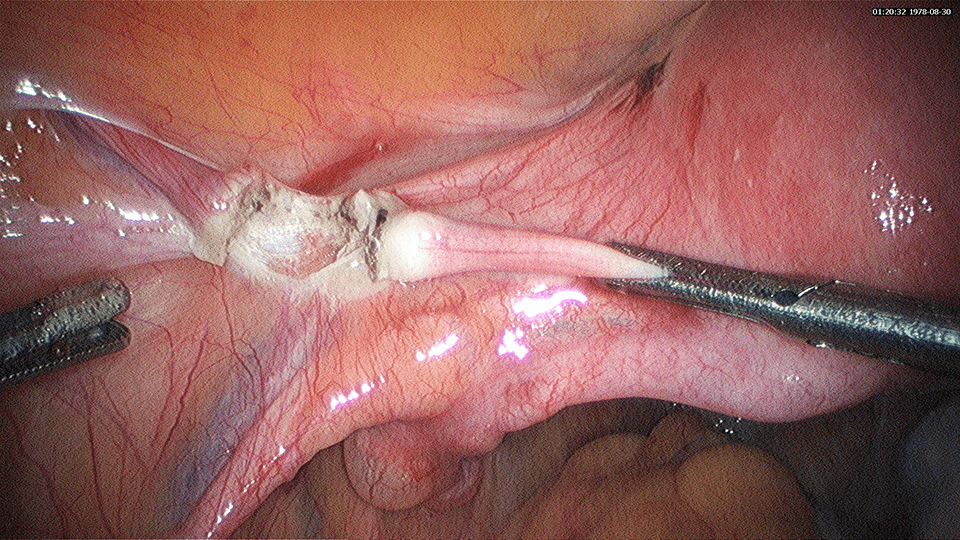
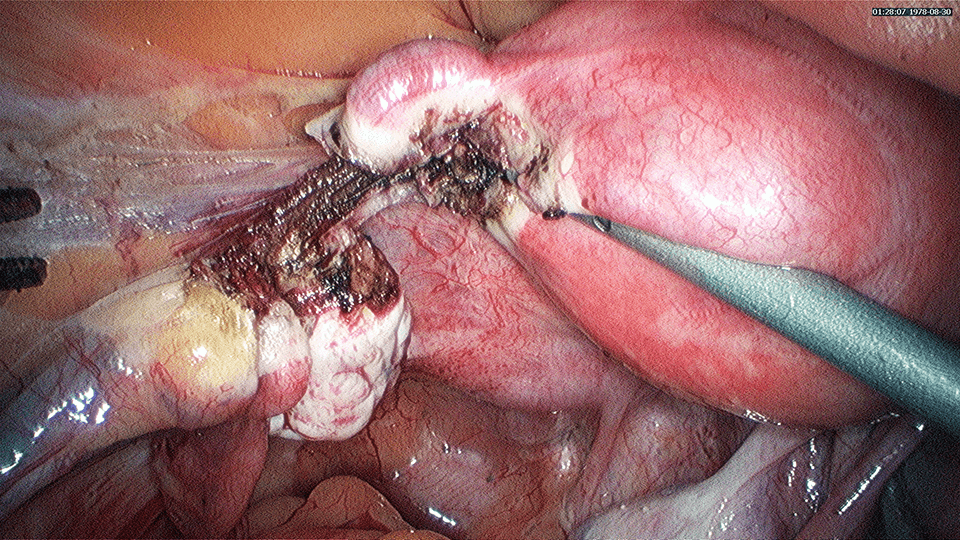
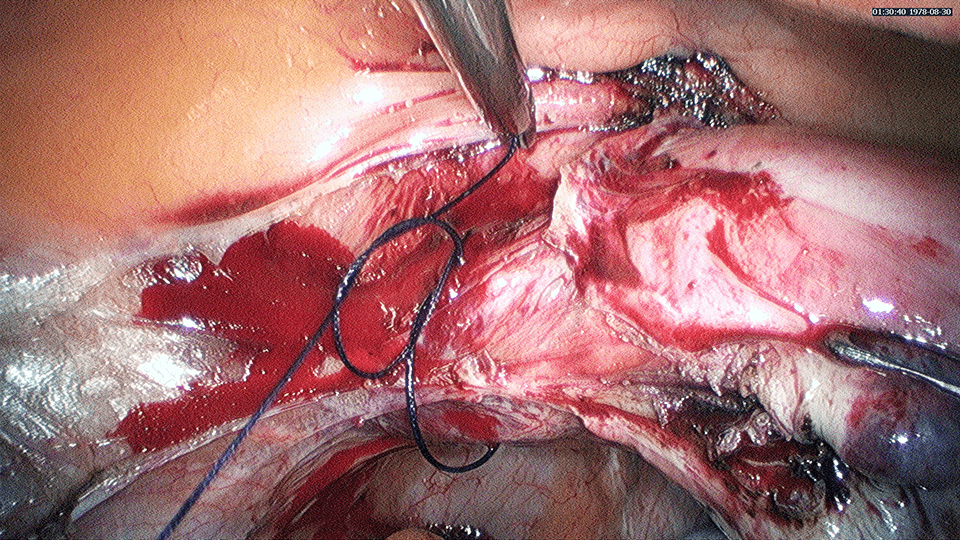
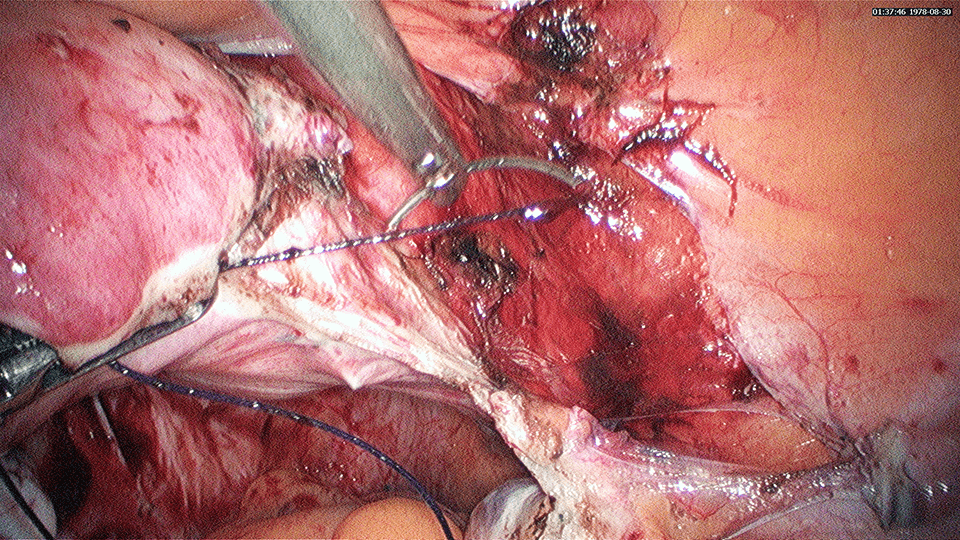
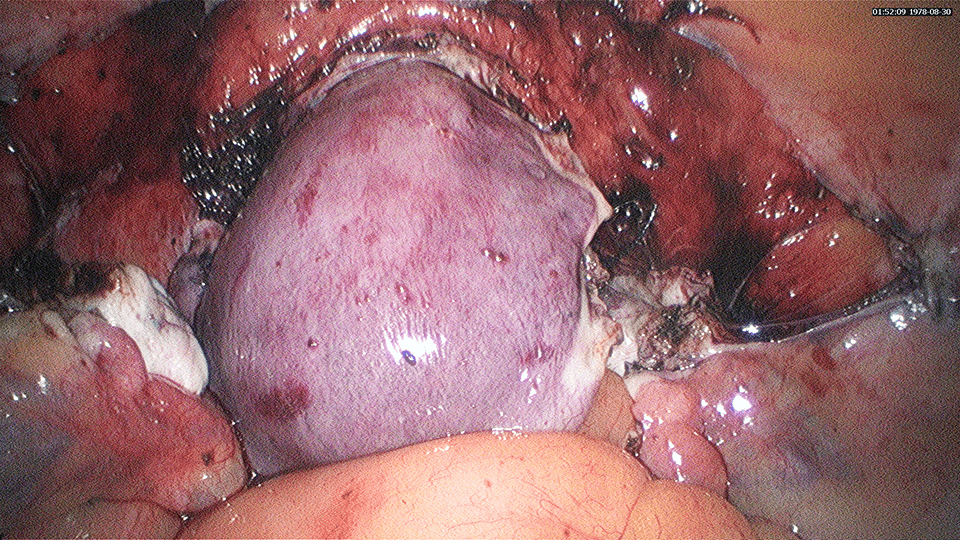
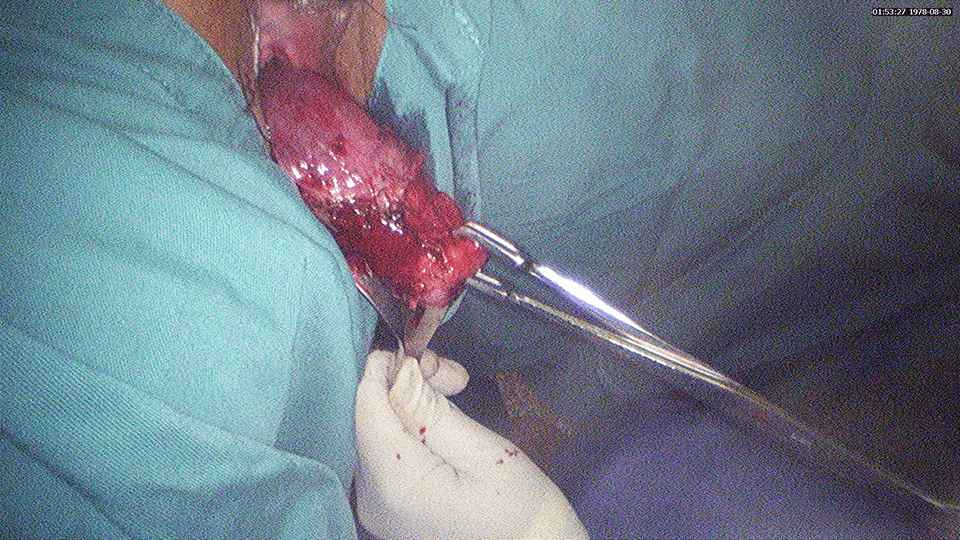
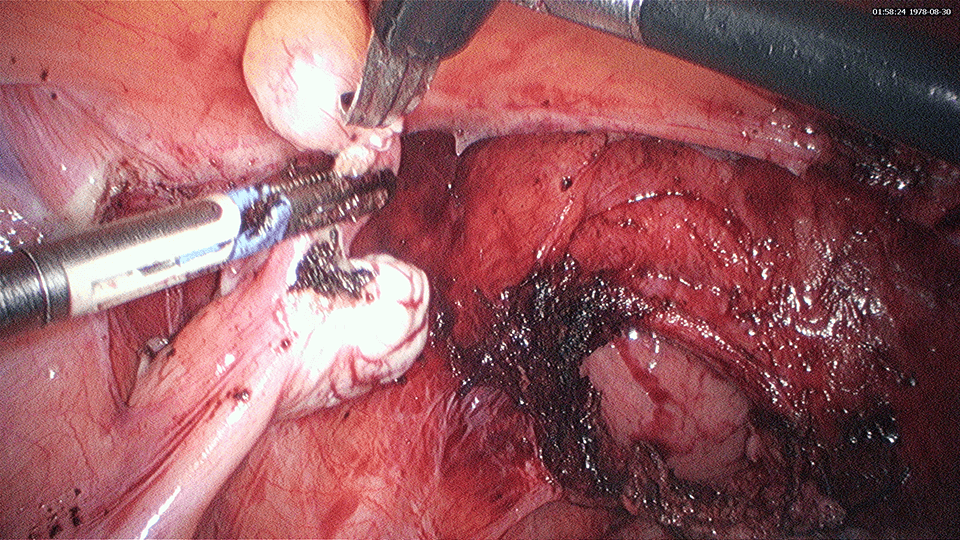
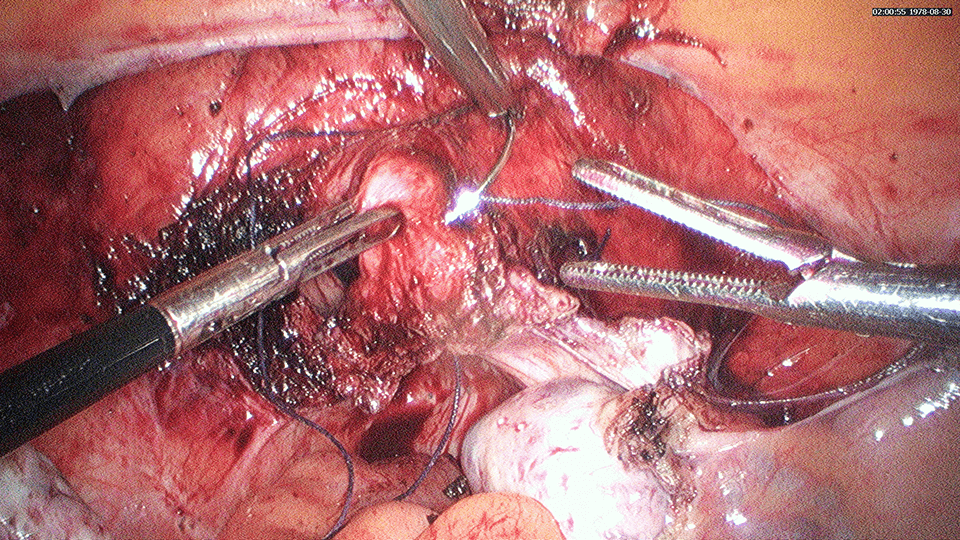
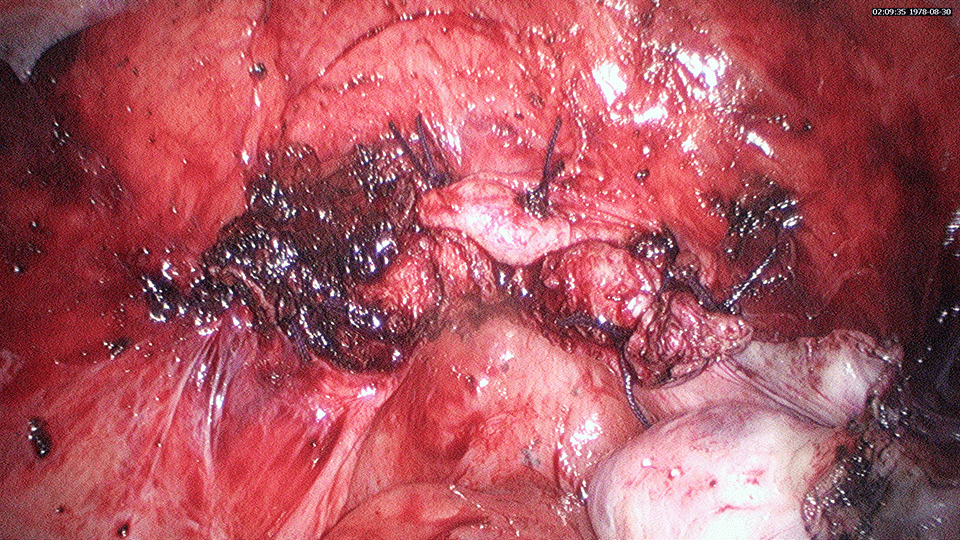
In diseases such as endometriosis, the bowel may be densely adherent (g) to the uterus, posteriorly. The bowel (rectum and sigmoid) may have to be released from the uterus and cervix before the hysterectomy can be performed. Accidental injury to the bowel may occur and the bowel will have to be repaired. If detected during surgery, the repair may be performed at the same time. However, if the injury is detected postoperatively then a second surgery may be necessary.
Again, the more experienced and skillful the surgeon is, the lesser the chances of developing complications.
Who are the candidates not suitable for Laparoscopic Hysterectomy?
Not all women can benefit from a hysterectomy performed laparoscopically. The ability to perform a laparoscopic hysterectomy will depend on the skill of the surgeon. The more skillful the surgeon, the better his performance in complex laparoscopic cases, laparoscopically. It may be difficult to perform a surgery laparoscopically, in the following situations:
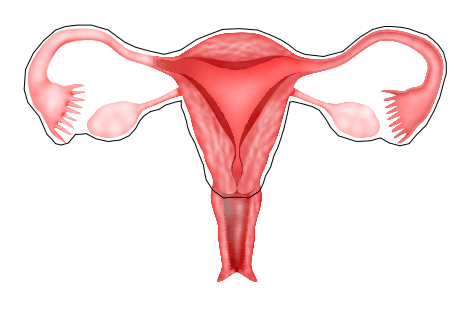
1) Large uterus
A uterus may be enlarged because of fibroids or adenomyosis. When the uterus is large, there may be less space for the surgeon to perform a Laparoscopic Hysterectomy. It may be difficult for a surgeon to visualize all the structures via a laparoscope. Sometimes, a GnRH (g) analogue injection may be given to shrink the fibroid before performing Laparoscopic Hysterectomy.
2) Multiple previous surgeries
Women who have undergone previous multiple open surgeries may have scar tissue (g) (adhesions) formed in the abdomen. These adhesions may cause the bowel to be adherent to each other and the uterus and the abdominal wall. It may be difficult to release these adhesions laparoscopically. Previous open surgeries are not an absolute contraindication for laparoscopic surgery. A skillful surgeon can place a laparoscope in the abdomen to see whether there are adhesions before deciding whether to proceed with the surgery laparoscopically or to convert to a laparotomy. Not all patients who have undergone previous surgeries may have scar tissue in the abdomen.
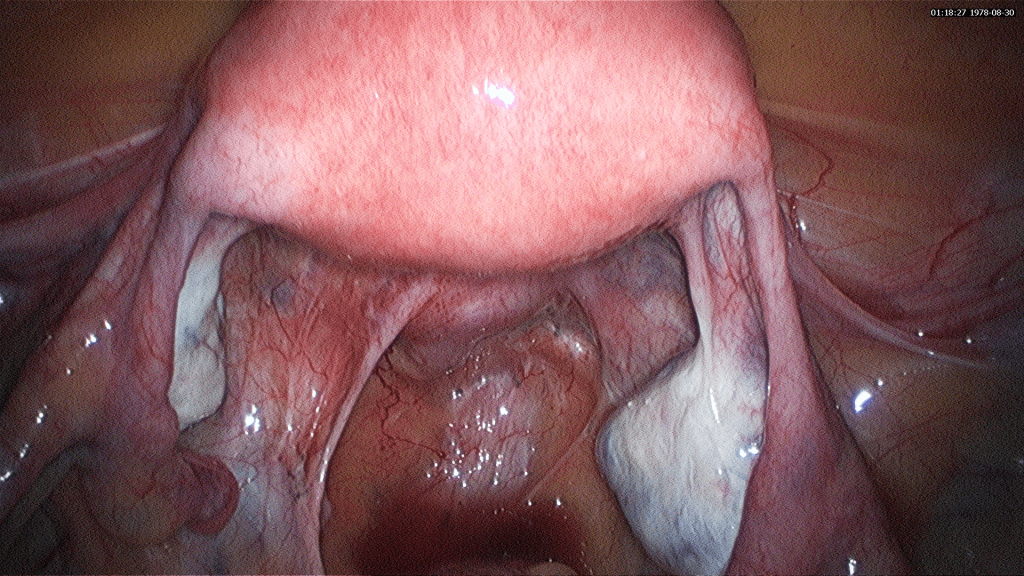
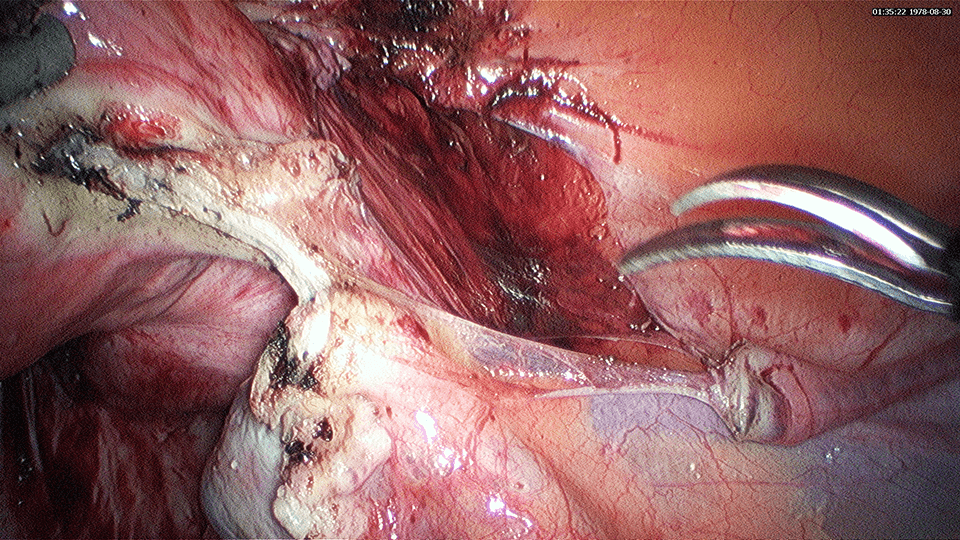
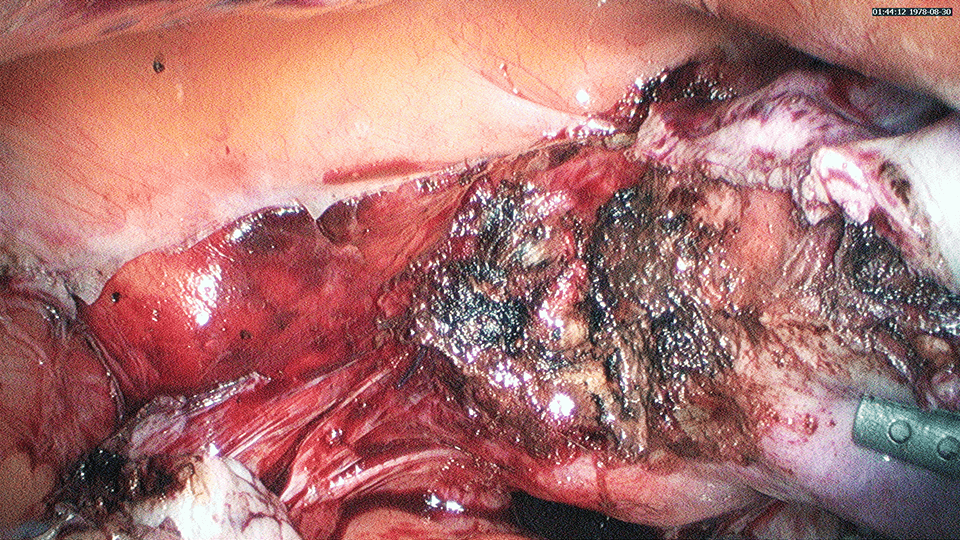
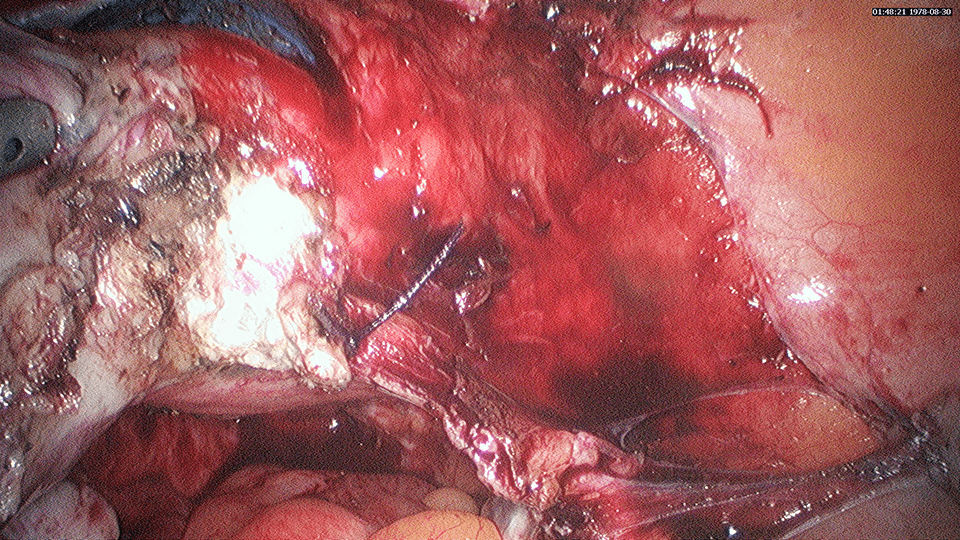
3) Severe adhesions as a result of endometriosis
Some patients with severe endometriosis may have severe adhesions of the uterus, ovaries and fallopian tubes to the pelvis. In such situations, the surgeon must be very skillful in dissecting away the adherent structures (ureters, bowel or bladder) from the uterus and pelvis before proceeding with the hysterectomy. Injury to these structures may require repair, which is easier to be performed by open surgery then by laparoscopy.