vNotes Hysterectomy
NOTES (Natural Orifice Transluminal Endoscopic Surgery) encompasses surgery performed via the stomach (transgastric), anus (transanal), urethra (transurethral) and vagina (transvaginal). Reddy and Rao et al performed the first transgastric appendectomy in humans using a flexible endoscope (1). The use of transgastric, transanal and transureteral approach is not as popular as the transvaginal approach. Many surgeries have been performed by the transvaginal route namely cholecystectomy, appendectomy, sigmoidectomy, nephrectomy, splenetomy, liver resection and sleeve gastrectomy in bariatic surgery. In gynaecology it has been used for salpingectomy (3), Ovarian cystectomy (4), myomectomy (5). Hysterectomy (2), lymphadectomy (6) and sacrocolpopexy (7). In 2012 , Su et all reported the first vNOTES hysterectomy through a posterior colpotomy in 16 patients with benign uterine diseases (2). Since then vNOTES especially hysterectomy is getting more popular.
Asia Pacific Association of Gynaecological Endoscopy Society organises vNOTES workshops. I attended the 2nd workshop last year in Bangkok. It was a 3 days hands-on workshop. We were taught how to perform vNOTES hysterectomy. Having attained this skill I started performing vNOTES hysterectomies in April 2019. So far I have performed 29 vNOTES hysterectomies.
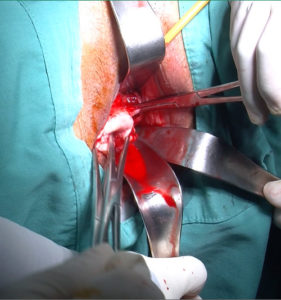
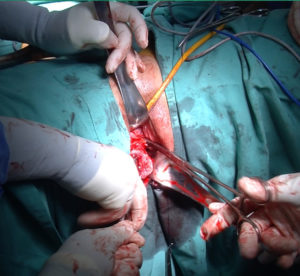
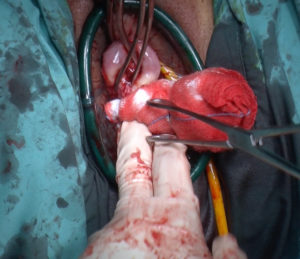
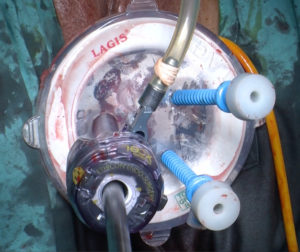
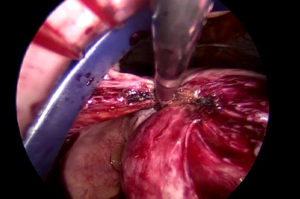
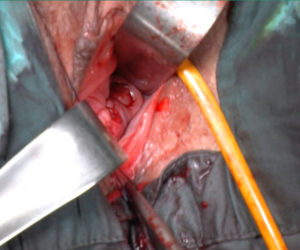
The surgery commences with first infiltrating the cervix with diluted adrenaline. Then a circumferential incision is made around the cervix and the vagina is separated from the cervix. The uterosacral ligaments are clamped cut and sutured bilaterally and this brings down the cervix. Posterior colpotomy is performed and then the cardinals are clamped cut and ligated. Anterior colpotomy is performed. Sutures are placed on the peritoneum anteriorly and posteriorly. The uterines are then clamped cut and ligated. A Lagis wound retractor and lap base is placed. Trocars are placed and laparoscopy is performed . The upper pedicles which include the ovarian ligament and tubes or the infundibulopelvic ligaments are coagulated and cut. The uterus is then removed vaginally. Haemostasis is attained and the vaginal vault is then closed continuously. Cystoscopy is done to look for a jet of urine coming out of the ureteric orifices indicating uninjured ureters.
Selection of patients is important when starting to perform vNOTES. The best case to start of with is small uterus with no previous Caesarean Sections. It is also important to select cases with no adhesions in the POD because of the difficutly in performing a posterior culdotomy. In previosus Caesarean section cases the Lagis port is placed before the anterior colpotomy and the peritoneum is approached from the lateral position just above the uterine artery. This can be difficult and with practice, the flapping of the peritoneum can be seen to indicate that the peritoneum can be perforated.







Conclusion
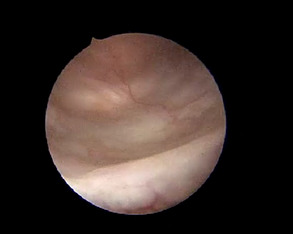
vNOTES can assist in converting a laparoscopic hysterectomy to vaginal hysterectomy. Performing laparoscopy vaginally need practice because the anatomy appears different from the vagina as opposed to conventional laparoscopy.
Reference
- Reddy N, Rao P.Per oral transgastric endoscopic appendectomy in human In: Paper Presented at 45th Annual Conference of Gastrointestinal Endoscopy of India, Jaipur, India. February 28e29 2004.
- Su H, Yen CF, Wu KY,Han CM, Le CL Hysterectomy via transvaginal natural orifice transluminal endoscopy surgery (NOOTES): feasibility of an innovative approach. Taiwan J Obstet Gynecol 2012;51:217e221
- Sarah VP, Jan B Natural orifice transluminal endoscopic surgery (NOTES) salpingectomy for ectopic pregnancy: a first series demonstrating how a new surgical technique can be applied in a low-resource setting. Gynecol Surg. 2015:12:299e302
- Wang CJ, W u PY, Kuo HH, Yu HT, Huang CY, Tseng HT. Natureal orifice transluminal endoscopic surgery-assisted versus laparoscopic ovarian cystectomy (NAOC vs LOC): A case-matched study. Surg Endosc. 206 :30;122731234
- Liu J, Lin Q, Blazek K, Liang B, Guan X. Transvaginal natural orifice transluminal endoscopic surgery myomectomy: a novel route for uterine myoma removal. J Minim Invasive Gynecol 2018:25:959e960
- Lebanc E, Narducci F, BressonI, Hudry D. Flurescence assisted sentinel (SND) and pelvic node dissection by singleport transvaginal laparosopic surgery for management of an endometrial carcinoma (EC) in an elderly obese patient Gynecol Oncol 2016;143:686e687
- Chen Y, Li J, Zhang Y, Hua K. Transvaginal single-port laparoscopy sacrocolpopexy. J Minim Invasive Gyneclo. 2018:25z;585e588
Selva
Sevellaraja Supermaniam
22/02/2021