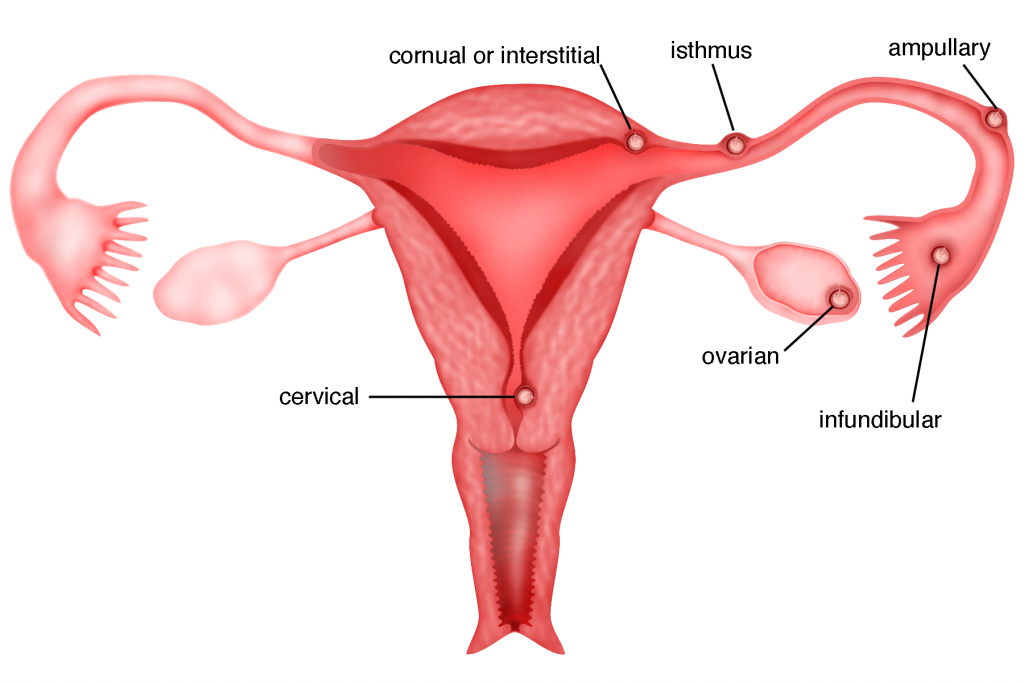
An ectopic pregnancy occurs when a fertilised egg settles and grows as a pregnancy in any location other than the inner lining of the uterus. As these other locations are not expandable as the uterus, when the pregnancy grows, it may cause these areas to rupture and bleed. The most common site for an ectopic pregnancy is the fallopian tube (98%) and so it is commonly called a tubal pregnancy. Tubal pregnancies can grow in the infundibular and fimbrial end (5% of all ectopics), the ampullary section (80%), the isthmus (12%), and the cornual and interstitial part of the tube (2%). However, they can also occur in other locations such as the ovary, cervix, and abdominal cavity. An ectopic pregnancy occurs in about one in 50 pregnancies.
Ectopic Pregnancy is a medical emergency and can be life threatening. It can rupture leading to internal bleeding. Ectopic pregnancy must be diagnosed and treated early because severe bleeding can lead to death. The pregnancy itself rarely survives and it cannot be moved into the uterus. Ectopic pregnancy remains the leading cause of pregnancy- related deaths in the first trimester of pregnancy.
In rare cases, an ectopic pregnancy may occur at the same time as an intrauterine pregnancy. This is referred to as heterotrophic pregnancy.
Risk factors for ectopic pregnancy
A normal pregnancy occus when the egg and sperm meet in the fallopian tube. The resulting embryo needs to travel to the uterus before implanting on the lining of the uterus. Anything that interferes with this can cause an ectopic pregnancy.
Ectopic pregnancy occurs when there is a disruption in the normal anatomy of the fallopian tubes. The inner lining of the fallopian tube is coated with hair-like projections called the cilia. Transport of the oocytes (eggs) and the embryo, from the fimbrial end to the uterine cavity is aided by these cilia. If these cilia are damaged, proper transport will be disrupted, and this may lead to an embryo not being able to reach the uterine cavity and therefore may attach itself to the fallopian tube leading to an ectopic pregnancy. Some risk factors involved are:
1) Patients who have had ectopic pregnancies before have the highest risk of developing more ectopic pregnancies.
2) Congenital abnormalities of the fallopian tube can cause abnormal implantation of the embryo leading to an ectopic pregnancy.
3) Surgery to the fallopian tube such as tubal ligation and repair of the fallopian tubes can lead to scarring and disruption of the normal anatomy of the tubes and increases the risk of an ectopic pregnancy.
4) Infection in the pelvis (pelvic inflammatory disease) is another risk factor for ectopic pregnancy. Sexually-transmitted diseases such as gonorrhoea and clamydia can cause damage to the inner lining of the fallopian tube leading to an ectopic pregnancy. Women with multiple sexual partners have a higher risk of sexually transmitted diseases and so may have a higher incidence of ectopic pregnancy.
5) The presence of endometriosis, fibroids and pelvic adhesions (scar tissue) can cause narrowing of the fallopian tubes. This may lead to disruption of the transport of an embryo, leading to implantation in the fallopian tube.
6) Intrauterine contraceptive device (IUCD) is effective in reducing the incidence of intrauterine pregnancy but not ectopic pregnancy. As such, if a patient were to conceive with an IUCD, she would have a higher chance of having an ectopic pregnancy. However, the incidence of pregnancy with IUCDs is very low.
7) Cigarette smoking around the time of conception can affect ciliary movement and has also been associated with an increased risk of ectopic pregnancy. This risk was observed to be dose-dependent, which means that the risk is dependent upon the individual woman’s habits and increases with the number of cigarettes smoked.
However, it is important to note that ectopic pregnancy may occur in women with none of the risk factors above.
Signs and Symptoms
The classic signs and symptoms of ectopic pregnancy include:
1) The Absence of Menstrual Periods (amenorrhoea)
2) Unusual Vaginal Bleeding
The bleeding can be either heavier or lighter than the usual menses
3) Abdominal Pain
The pain is usually one sided and in the lower abdomen
The woman may not be aware that she is pregnant. The signs and symptoms of an ectopic pregnancy typically occur six to eight weeks after the last normal menstrual period, but they may occur later if the ectopic pregnancy is not located in the Fallopian tube. Other symptoms of pregnancy (for example, nausea and breast discomfort, etc.) may also be present in ectopic pregnancy.
If the ectopic pregnancy has ruptured, then the symptoms are as follows:
1) Sudden, severe lower abdominal pain spreading across the whole abdomen
2) Sweating, light headedness or feeling faint
3) Collapse or shock as a result of internal bleeding
4) Shoulder tip pain – this occurs as a result of internal bleeding that irritates the diaphragm (g).
Diagnosis of Ectopic pregnancy
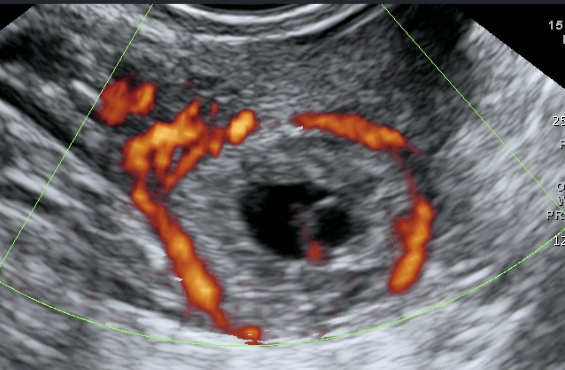
Diagnosis of ectopic pregnancy is made by first taking a good history from the patient followed by a pelvic examination and a transvaginal ultrasound. Due to irregular pervaginal bleeding, some patients may not even know that they are pregnant. The patient may have abdominal tenderness (tummy pain). Pelvic examination may reveal tenderness and bogginess (sponginess due to high fluid content) at the posterior part of the cervix. A pelvic mass may be felt during pelvic examination. A urine pregnancy and/or a serum beta HCG test (the beta subunit of human chorionic gonadotrophin) is necessary to confirm pregnancy. Transvaginal ultrasound is the most useful test to visualise an ectopic pregnancy. In this test, an ultrasound probe is inserted into the vagina, and pelvic images are visible on a monitor. Usually there will not be a gestational sac in the uterine cavity leading to a suspicion of an ectopic pregnancy. Transvaginal ultrasound may reveal an ectopic gestational sac near the ovary or in most situations, it may simply reveal a mass in the area of the fallopian tube raising the suspicion of an ectopic pregnancy. Some fluid will usually be seen in the posterior part of the uterus (Pouch of Douglas). When ectopic pregnancy is confirmed, then appropriate treatment will be suggested. However, when all the tests done are not confirmatory, a diagnostic laparoscopy may be necessary to visualise the structures in the abdomen and pelvis, thereby revealing the site of the ectopic pregnancy.
Health risk of an ectopic pregnancy
Spontaneous reabsorption of an ectopic pregnancy may occur. However, the true incidence of this occurring is unknown. It may not be possible to know in which patient the ectopic pregnancy may resolve spontaneously. Since ectopic pregnancy is located in places not intended for proper implantation of the embryo, rupture of the ectopic pregnancy may occur. The ectopic pregnancy may invade a vein or an artery, which can lead to bleeding. This can be life threatening and will require immediate surgery to remove the ectopic pregnancy. Another health risk is that blood in the pelvis can lead to adhesions and the scar tissue can lead to difficulty in conceiving in the future or increase the likelihood of future ectopic pregnancy.
Treatment options
Treatment options for ectopic pregnancy include observation, laparoscopy, laparotomy, and medication. Some ectopic pregnancies will resolve on their own without the need for any intervention. However, because of the risk of rupture most women who are diagnosed with ectopic pregnancy are treated with medication or surgery.
1) Surgery
There are 2 ways of performing surgery namely laparotomy and laparoscopy. Laparoscopy is the preferred method. However, in certain situations such as women with massive pelvic adhesions or when there is excessive bleeding, laparotomy may be performed. There are several ways of removing the ectopic pregnancy. In early unruptured ectopic pregnancies, a salpingostomy can be performed. Here, an incision is made in the fallopian tube and the ectopic pregnancy is removed, leaving the fallopian tube intact. However, if the tube has ruptured, it may be difficult to save the fallopian tube and removal of the fallopian tube (salpingectomy) may be necessary (see chapter 26).
Case 7.1 : Pregnant after laparoscopic surgery for ectopic pregnancy
Madam NM, a 32 year old lady, first saw me in May 2013. She was 7 weeks pregnant. Ultrasound showed 2 well formed intrauterine gestational sacs but no foetal heart activities were seen in either of the sacs, indicating that it was a miscarriage. She underwent an evacuation of the product of conceptus. Two months later she conceived again. Unfortunately, it was a left ectopic tubal pregnancy and she underwent a laparoscopic left salpingotomy in August 2013 (see video 26.2). She underwent a hysterosalpingogram (HSG) in November 2013. The right fallopian tube was patent (not blocked). Contrast (g) was seen in the left Fallopian tube but no spillage of contrast was seen from the fimbrial end. She could not conceive spontaneously after that and underwent an intrauterine insemination (IUI) (g) in April 2014. She conceived and delivered a baby girl.
2) Medical therapy
Medical treatment involves the use of an anti-cancer drug called methotrexate. This drug acts by killing the growing cells of the placenta, thereby inducing miscarriage of the ectopic pregnancy. This treatment is usually suggested in patients with early unruptured ectopic pregnancy. While on this treatment, the serial serum beta HCG test must be done. The treatment is considered effective if the levels are on a declining trend. The advantage of medical treatment is that the patient need not undergo surgery and will still have her fallopian tube. The disadvantage is that, in some patients, the ectopic pregnancy may not resolve and the patient may still need surgery. The worry is that rupture of the ectopic pregnancy may occur while on medication and this may require emergency surgery. A hysterosalpingography is usually done to assess the patency of the fallopian tube several months after successful treatment using methotrexate.
Prognosis – Future fertility
Fertility following ectopic pregnancy depends upon several factors, the most important of which is whether the patient has a prior history of infertility. The treatment choice, whether surgical or nonsurgical, also plays an important role. For example, the rate of intrauterine pregnancy may be higher following the methotrexate treatment compared to surgical treatment. The fertility rate may be better following salpingostomy rather than salpingectomy.

Summary
An ectopic pregnancy occurs when a fertilised egg settles and grows in any location other than the inner lining of the uterus. The most common site for an ectopic pregnancy is the fallopian tube. Ectopic pregnancy is a medical emergency. Diagnosis is usually made by a positive pregnancy test with the absence of an intrauterine gestational sac and a mass outside the uterine cavity. Treatment options include surgery and/or medical therapy.